Back to Blog

Pelvic floor exercises are often recommended as the first line of treatment for stress urinary incontinence. For many women, they can be highly effective.
However, one of the most common things we hear in the clinic is: “I’ve been doing my pelvic floor exercises, but I’m still leaking.”
If this sounds familiar, you’re not alone.
Many women feel frustrated, discouraged or even embarrassed when they don’t see the results they expected.
The good news is that in many cases, your technique isn’t wrong.
More often, women simply haven’t been given the right type of pelvic floor exercise for their specific presentation, haven’t been loading the muscles enough to create change, or require additional treatment options alongside their pelvic floor exercises.
Pelvic floor strength is important, but it is not the whole story.
As we discussed in Part 1 of this series, stress urinary incontinence (SUI) can occur for different reasons. Some women have a support problem, some have a urethral sphincter problem, and many have a combination of both. Understanding why you are leaking is often the key to understanding why your current treatment hasn’t worked.
In this blog, we’ll explore the most common reasons pelvic floor exercises don’t achieve the desired outcome, how pregnancy, childbirth, menopause and hormonal changes can influence leakage, and why assessment is so important.
Not All Pelvic Floor Exercises Train the Same Thing
One of the biggest misconceptions about pelvic floor exercises is that there is one exercise program that works for everyone.
In reality, different women leak for different reasons.
Some women have a support problem, where the bladder and urethra move excessively during activities such as coughing, sneezing or running.
Others have a sphincter problem, where the urethral sphincter isn’t generating enough closure pressure.
Some women have a combination of both.
The exercises prescribed for these different presentations may look quite different.
For example, one woman may benefit from improving the support provided by the larger levator ani muscles, while another may require more specific training aimed at improving urethral sphincter function.
This is one reason generic pelvic floor programs don’t always work.
Your Exercises Might Not Be Challenging Enough
This is one of the most common things we see in clinic.
Like every other muscle in the body, the pelvic floor needs to be challenged to become stronger.
If you don’t challenge a muscle, you can’t expect it to change.
Many women are prescribed exercise programs that are simply not difficult enough to create adaptation.
Think about strengthening your biceps.
Completing five easy curls with a light weight every day is unlikely to create significant strength gains.
The pelvic floor is no different.
To become stronger, the muscles need to be loaded appropriately and progressively challenged over time.
When performing a strengthening program, the final repetitions should feel difficult.
You should be working towards fatigue.
As I often tell patients, by the end of your exercises you should be glad you don’t have to do any more.
Your Exercises May Not Have Been Progressed
Many women are given a pelvic floor program and continue performing exactly the same exercises for months or even years.
The body adapts quickly.
As strength improves, the exercises need to become more challenging.
Progression may involve:
- Increasing hold times
- Increasing repetitions
- Increasing training frequency
- Improving endurance
- Increasing contraction speed
- Adding functional positions
- Adding exercise-specific tasks
- Introducing impact and loading
Without progression, results can plateau.
Pelvic Floor Strength Is Not the Only Answer
One of the biggest messages we hope women take away from this series is that leakage is not always a simple strength problem.
You may have:
- Reduced support around the bladder and urethra
- Urethral sphincter weakness
- Hormonal influences
- Pregnancy-related changes
- Childbirth-related changes
- Pelvic organ prolapse
- Connective tissue changes
In these situations, strengthening alone may not fully address the problem.
Additional treatment strategies are often required.
Pregnancy Can Change the Support System
Many women are surprised to develop stress urinary incontinence during pregnancy, even if they have never leaked before.
Pregnancy creates significant changes within the continence system, even before birth occurs.
One of the major changes relates to oestrogen.
Higher levels of oestrogen help prepare the body for pregnancy and birth by increasing the flexibility of connective tissues and fascia throughout the pelvis.
While this increased flexibility is important for birth preparation, it can also reduce the stiffness of the support structures around the bladder and urethra.
As these support structures become more flexible, the bladder may move more during activities such as coughing, sneezing and exercise.
At the same time, the growing baby increases the load placed on the pelvic floor muscles.
The pelvic floor therefore has to work harder to provide the same level of support.
For some women, this combination of increased load and reduced support can contribute to leakage.
It is important to remember that developing stress urinary incontinence during pregnancy does not automatically mean your pelvic floor is weak. Often, the pelvic floor is simply being asked to manage greater loads while working with more flexible support structures.
Childbirth Can Affect More Than Strength
After childbirth, many women assume leakage means their pelvic floor has become weak.
While strength can certainly be affected, childbirth can influence several parts of the continence system.
Potential contributors include:
- Stretching of the pelvic floor muscles
- Injury to the support structures around the bladder and urethra
- Changes to connective tissue support
- Temporary nerve irritation
- Reduced urethral sphincter function
For some women, symptoms improve significantly within the first six to twelve months postpartum as tissues continue to recover.
For others, additional support and rehabilitation may be required.
This is why a postnatal pelvic floor assessment can be so valuable.
Menopause Can Affect Continence in Several Ways
Many women notice stress urinary incontinence for the first time during perimenopause or menopause.
This is not simply because of ageing.
Declining oestrogen levels can influence multiple parts of the continence system.
Impact on the Urethral Sphincter
Oestrogen helps maintain the health of the tissues that contribute to urethral closure pressure.
As oestrogen levels decline:
- Blood flow around the urethra may reduce
- The tissues around the urethra may become thinner
- Urethral closure pressure may decrease
- The urethral sphincter may become less effective at maintaining continence
For some women, this reduction in closure pressure is enough to trigger leakage.
Impact on the Pelvic Floor Muscles
Like all muscles in the body, the pelvic floor can be affected by hormonal changes and ageing.
Some women notice a reduction in pelvic floor strength, endurance and responsiveness during and after menopause.
This may reduce the ability of the pelvic floor to provide adequate support during sudden increases in pressure.
Impact on the Fascia and Support Structures
The fascia and connective tissues that support the bladder and urethra can also become less resilient over time.
When these support structures become less effective, the bladder and urethra may move more during coughing, sneezing and exercise.
This can contribute to reduced support and increase the likelihood of leakage.
For many women, menopause-related stress urinary incontinence is caused by a combination of reduced support and reduced urethral closure pressure.
The good news is that there are treatment options available, and many women experience significant improvement with the right combination of physiotherapy, strength training, support devices and, where appropriate, vaginal oestrogen therapy.
Why Does Leakage Change Throughout the Menstrual Cycle?
Some women notice that their leakage changes throughout the month.
You may feel stronger and more supported during some phases of your cycle and notice increased leakage during others.
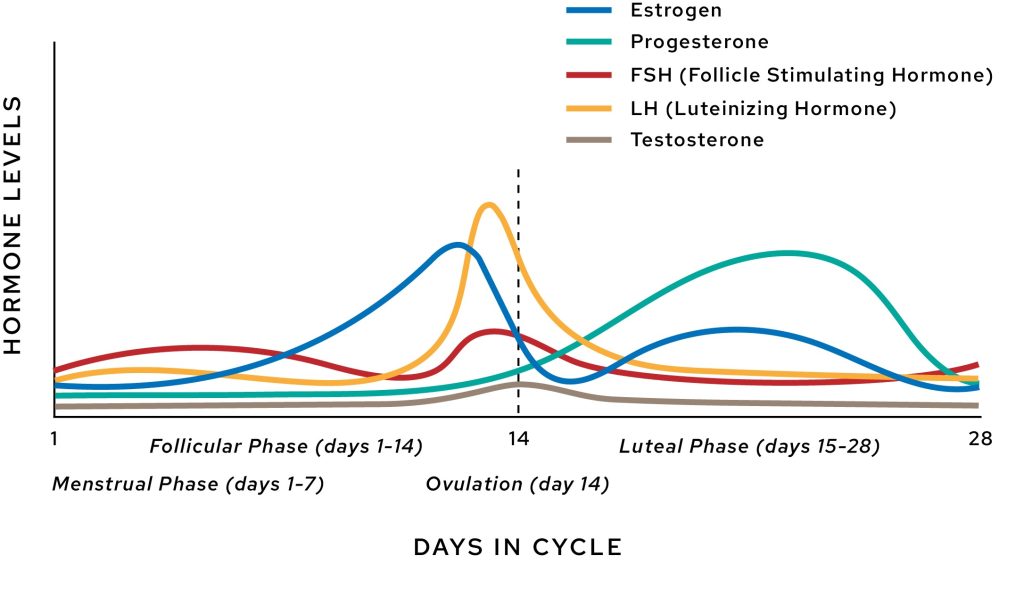
Changes in oestrogen levels throughout the menstrual cycle can influence the tissues that help support continence.
Around ovulation, oestrogen levels peak. During this phase, connective tissues and fascia tend to become more flexible. While this is a normal and healthy physiological response, some women may notice slightly less support around the bladder and urethra, which can contribute to increased leakage.
In the days leading up to and during menstruation, oestrogen levels fall significantly. Lower oestrogen levels can temporarily reduce urethral closure pressure and the effectiveness of the tissues surrounding the urethra. Some women notice increased leakage during this phase because the urethral sphincter and surrounding tissues are not able to generate the same level of closure pressure.
This does not mean your pelvic floor has suddenly become weak.
Rather, it reflects the normal influence that changing hormone levels can have on the continence system.
If you notice a clear pattern to your leakage across your cycle, this can be valuable information to discuss with your pelvic floor physiotherapist.
What Happens During a Pelvic Floor Physiotherapy Assessment?
One of the biggest benefits of seeing a pelvic floor physiotherapist is that we aim to understand why you are leaking.
Your assessment may include:
- Discussion of your symptoms
- Pregnancy and birth history
- Exercise and sporting history
- Menopause and hormonal considerations
- Bladder habits
- Pelvic floor assessment
- Assessment of support structures
- Assessment of urethral sphincter function
- Real-time ultrasound assessment
This information helps guide treatment and identify which strategies are most likely to be beneficial.
Finding the Real Cause
If you’ve been doing pelvic floor exercises and haven’t seen the results you hoped for, it doesn’t necessarily mean physiotherapy won’t help.
It may simply mean the underlying cause of your leakage hasn’t yet been identified.
Rather than asking:
“How can I strengthen my pelvic floor?”
a more helpful question is often:
“Why am I leaking?”
Once that question is answered, treatment can become far more targeted and effective.
In Part 3 of this series, we’ll explore the many treatment options available for stress urinary incontinence, including pelvic floor muscle training, vaginal weights, electrical stimulation, pessaries and continence support devices.
Book an Appointment
If you’re experiencing leakage despite performing pelvic floor exercises, our women’s health physiotherapists can help identify why it is happening and develop a treatment plan tailored to your specific presentation.
Book online via our website (Book Now) or call us on (03) 8828 4761 to speak with our team and arrange an appointment.
Learn more about how pelvic floor physiotherapy may support your recovery.